
<p>Karina Mendoza-Valdez, a registered nurse, rolled up her sleeve and smiled at Courtney Senechal before she administered the Moderna vaccine at East Boston Neighborhood Health Center in East Boston on December 21, 2020. Health care workers at East Boston Neighborhood Health Center were believed to be among the first in Massachusetts to receive a vaccine developed by Moderna. (Photo by Jessica Rinaldi/The Boston Globe via Getty Images)</p>
In mid-December, health care workers across the United States began to receive a COVID-19 vaccine. These workers have faced constant exposure to COVID-19 as they’ve struggled to provide care amid the pandemic, making them the top priority for receiving the vaccine.
With vaccine production still underway, the Advisory Committee on Immunization Practices has identified who it considers the next priority: adults ages 75 and older and a third of the essential workforce that faces greater risk of contracting COVID-19, including first responders and workers involved in education, manufacturing, corrections, public transit, grocery sales, food and agriculture, and the US Postal Service. The 57 million essential workers in other industries and workers in nonessential industries, many of whom work in close proximity to others, will not receive vaccines until production increases.
The COVID-19 pandemic is far from over, yet in most areas, many businesses are open. As a result, workers in both essential and nonessential industries face varying exposure to the coronavirus. In a new report, we use the 2018 American Community survey to examine the potential coronavirus exposure risks faced at work. We find Black, Native American, and Hispanic/Latinx workers are more likely to work in person and in close proximity to others, putting them at greater risk of contracting COVID-19.
Black, Native American, and Hispanic/Latinx workers face greater coronavirus exposure risks in the workplace
Since COVID-19 began to spread in the US, many workers have not been able to transition to remote work. Despite their importance to society and the risks they bear, workers who must work in person and in close proximity to others have lower incomes and greater likelihood of being uninsured. These workers, who both are more susceptible to contracting COVID-19 and have fewer resources for health care and isolation costs, are disproportionately likely to be Black, Native American, or Hispanic/Latinx.
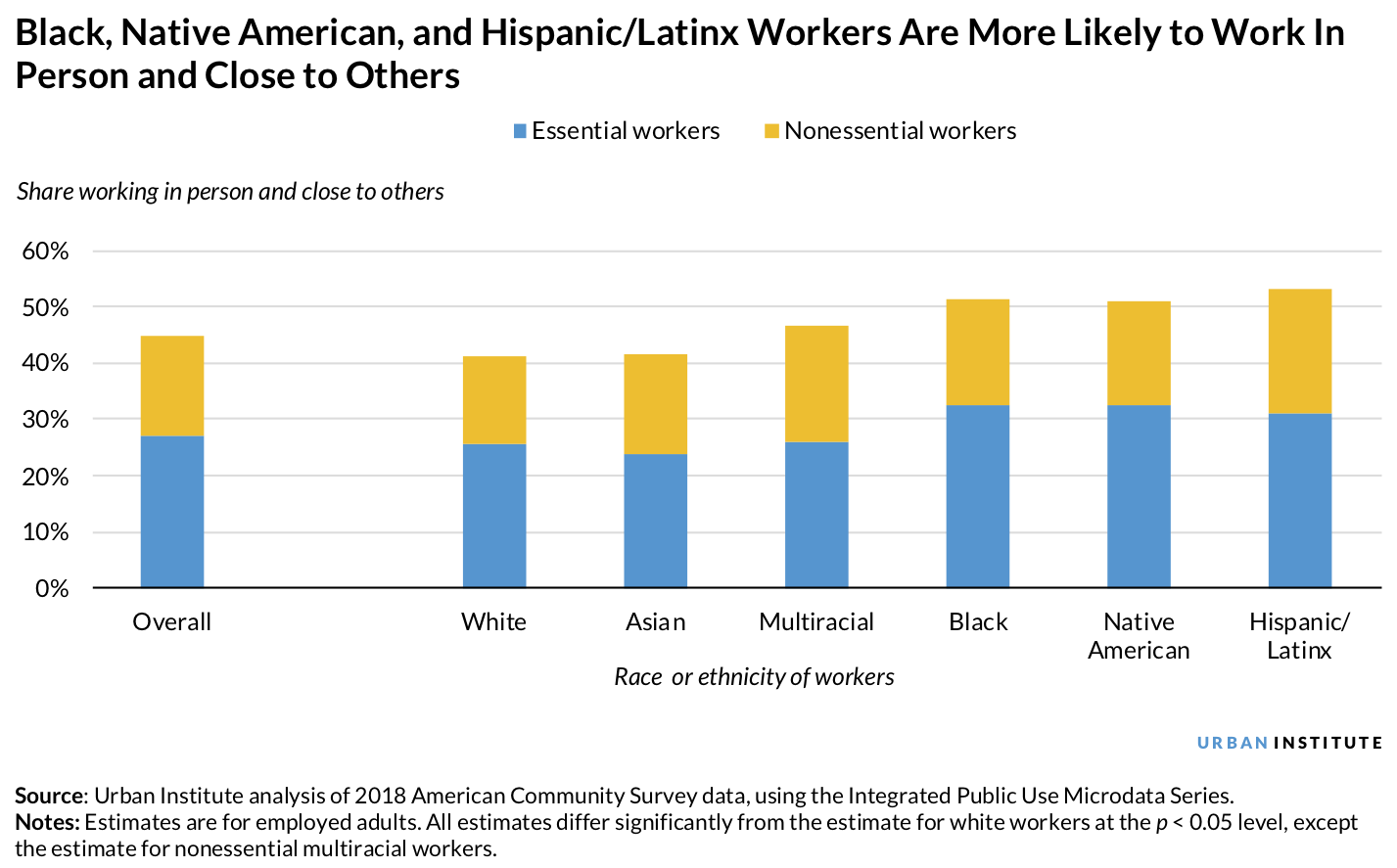
A third of Black, Native American, and Hispanic/Latinx workers had essential jobs that require them to work in person and close to others, compared with just a quarter of white workers. Black, Native American, and Hispanic/Latinx workers are also more likely than white workers to work in person and close to others in nonessential industries. Altogether, more than half of Black, Native American, and Hispanic/Latinx workers had jobs that must be done in person and that required working in close proximity to others.
Structural and interpersonal racism in the US has limited and excluded people of color from opportunities, with Native American, Black, Asian, and Hispanic/Latinx people each experiencing unique forms of oppression. These structural factors have permeated all aspects of life, affecting access to homes, health care, education, and employment and have contributed to profound differences in the occupations of white workers relative to other groups. These occupational differences mean that Black, Native American, and Hispanic/Latinx workers are more likely than white workers to risk exposure to the coronavirus in the workplace, which has likely contributed to greater case and mortality rates and more economic hardship.
Reducing the disparate burden of COVID-19 on Black, Native American, and Hispanic/Latinx workers
To decide which groups should have priority in receiving the vaccine, the Centers for Disease Control and Prevention stated that one goal of vaccination allocation is to “reduce the extra burden the disease is having on people already facing disparities.” This analysis shows that getting vaccines to workers who must work in person and in close proximity to others would help achieve that goal. Black, Native American, and Hispanic/Latinx workers are overrepresented among those who face higher risk of exposure in the workplace. And the advisory committee has not addressed nonessential workers facing similar risks.
The COVID-19 vaccine will eventually protect the health of workers who cannot work from home, particularly those who work closely with others, but it is just one of many public health tools available to governments. Communities and states can and should take other steps right now to protect exposed workers who are not yet eligible for the vaccine and reduce community transmission rates.
- Protect workers by enacting public health practices that reduce transmission risk. Communities can reduce risks for workers by enacting face-covering and social distancing regulations, limiting indoor events and capacity, and providing affordable, quick testing and timely contact tracing. These measures are increasingly important given the more transmissible coronavirus variant now in the US.
- Renew and Broaden the Families First Coronavirus Response Act’s paid sick leave provisions. To protect more workers, the paid sick leave mandates must be renewed and can be expanded to firms with more than 500 employees, the number of paid hours can be increased, and sick leave can be provided to gig workers so they can isolate if they are exposed or sick.
- Enact and enforce workplace practices. Policymakers can require employers to reduce risks for their employees by ensuring workers are at least six feet from colleagues and customers when possible, providing and requiring face coverings indoors, increasing ventilation, installing appropriate filters in shared spaces, providing employees with regular access to handwashing, and notifying workers when cases are reported.
For states to reduce transmission risks before the vaccine reaches workers who need to work in person and close to others, they will need to enact these public health and workplace safety measures to protect workers and their families. Although these policy and workplace changes will help protect the people currently keeping society running, they do not address the policies and practices that produce the racial and ethnic inequities putting them at increased risk. Eliminating these inequities will require comprehensive changes that address their root causes.
The authors are grateful to Rayna Phelps for her help with state vaccination plan research.
Let’s help communities build more secure, hopeful futures.
Today’s complex challenges demand smarter solutions. Urban brings decades of expertise to understanding the forces shaping people’s lives and the systems that support them. With rigorous analysis and hands-on guidance, we help leaders across the country design, test, and scale solutions that build pathways for greater opportunity.
Your support makes this possible.