
<p>In this Wednesday, April 13, 2016 photo, Herbert Diamond, 88, left, of Fort Lee, N.J., speaks with Dr. Manisha Parulekar about his end of life preferences, at the Hackensack Medical Center in Hackensack, N.J. Such conversations, are slowly spreading across the U.S. as Medicare rolls out government payments for the consultations. Photo by Julio Cortez/AP</p>
A version of this post originally appeared on Health Affairs.
From all the political discussion about health care, you’d think that government health policy lives or dies by what happens to the Affordable Care Act, or Obamacare. One side offers almost nothing apart from saying Obamacare must (somehow) be abandoned. The other side tells us that health costs, partly thanks to Obamacare, might be under control. Neither side faces up to the continuing dominance of health costs in projections of future federal spending.
Meanwhile, a recent study suggests yet again that spending much more on health care may do little to improve mortality and opportunity for the disadvantaged.
Like most debates that become political, the discussion tends to be numberless. Numbers aren’t always popular for those whose facts must fit their storylines, as opposed to those whose storylines evolve from the facts.
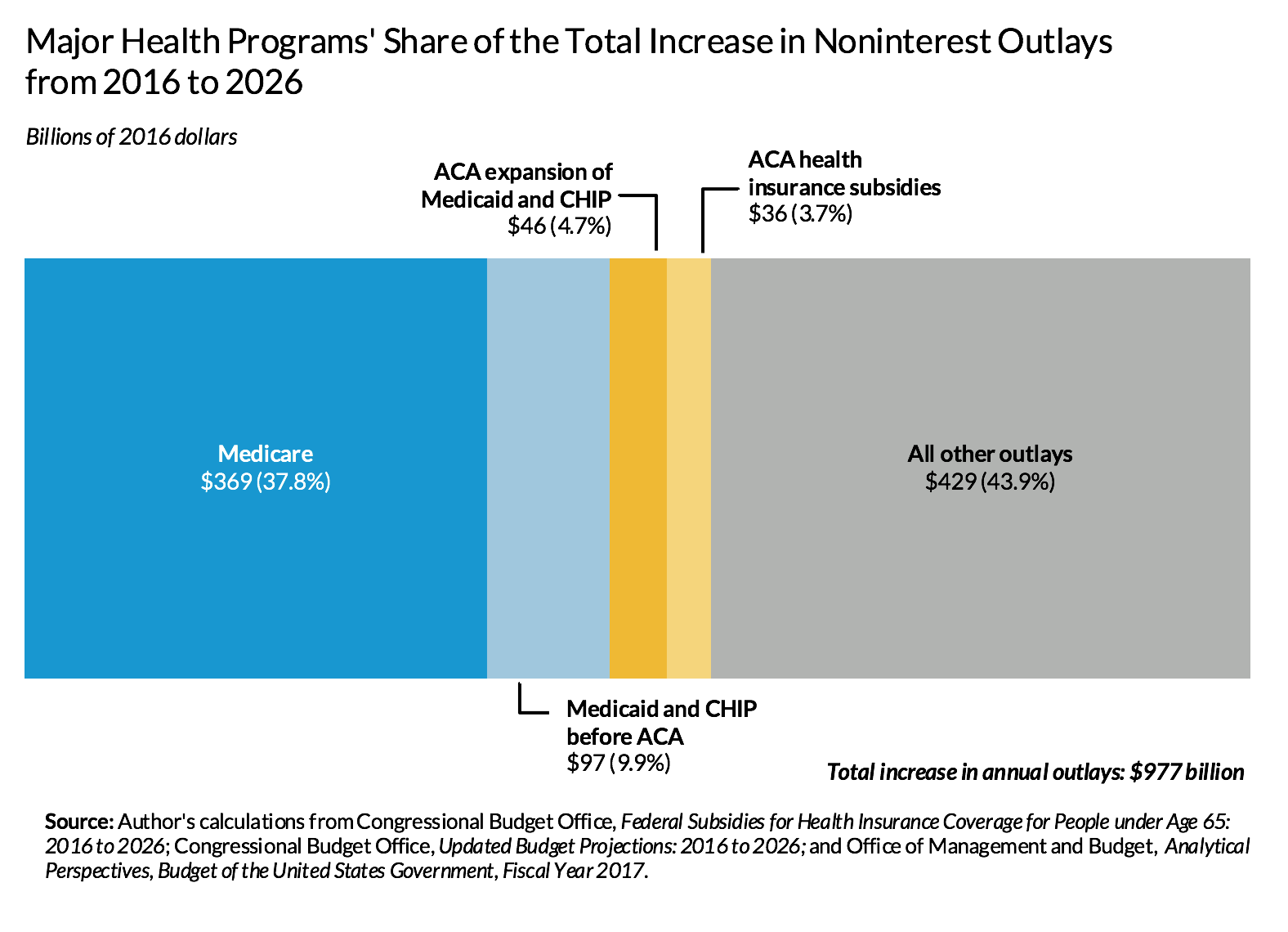
So what do the numbers tell us? Figure 1 shows that health care spending composes most of all projected increases in noninterest outlays of the federal government, but that Obamacare for those under age 65 is only a moderate cause of this growth.
Note: Because I focus on health costs, not on how we pay for them, calculations exclude payments made by taxpayers to support these programs, such as Medicare Part B premiums that budget analysts sometimes net from gross outlay payments. Allocation of costs or changes in costs over time because of Obamacare may exclude potential secondary impacts, such as a shift out of employer-provided health care or a change in Medicaid costs for people over age 64.
The health spending problem is still with us
Despite slower health spending growth, we have not solved our health spending problem. In 2026, the federal government is expected to spend (and subsidize through the employer coverage tax exclusion) at least $693 billion (in 2016 dollars) more than today for major health insurance programs. If we exclude the tax subsidies (as the exhibit does), this sum decreases, but only to $548 billion.
Excluding interest on debt, federal outlays for major health programs (excluding tax subsidies, which aren’t counted in outlays) eat up around 29 percent of today’s total federal outlays but about twice as much—56 percent—of the growth in total outlays between now and 2026 (figure 1).
Turning to the economy more broadly, for every additional dollar of real gross domestic product per capita expected 10 years from now, 20 cents will go toward supporting the rise in federal health insurance programs costs. And even these numbers significantly understate growth in total health costs by leaving out state and local health costs, other federal costs such as health research, and private spending on health care. Adding these other costs would indicate that health care continues to eat up a very large fraction of economic growth. Much of the confusion here about whether “health cost growth has slowed” occurs because lower economic growth tends to reduce the growth rate of all spending items, including health care, but not necessarily the share of growth absorbed by health care.
The relatively minor role of Obamacare
Obamacare has very little to do with any of this. If we include growth in tax subsidies for health insurance, Obamacare programs for those younger than 65, including Medicaid expansion and new health insurance subsidies in the Marketplace, entail only about 8 percent of the federal government’s cost for major health programs and 12 percent of the projected increase in annual cost within a decade. And even those additional Obamacare costs are offset partly by cuts established in the Affordable Care Act.
In contrast, growth in Medicare makes up half or more of all federal major health program spending and of the projected increases; the tax break for employer-provided insurance and the Medicaid program for those eligible before Obamacare also entail significantly higher costs than does Obamacare.
Moving forward
We have a long way to go in reforming health care and health care costs. Such reform must tackle all elements of what I have labeled our four-tranche system of federal subsidies: Medicare, Medicaid, employment-based subsidies, and the exchange subsidies established in Obamacare. We must also remember that the goal of reform is not simply to reduce costs but to shift resources to where public gains are expected to be higher, including preventing health problems before they arise.
Copyright ©2015 Health Affairs by Project HOPE – The People-to-People Health Foundation, Inc.
Let’s help communities build more secure, hopeful futures.
Today’s complex challenges demand smarter solutions. Urban brings decades of expertise to understanding the forces shaping people’s lives and the systems that support them. With rigorous analysis and hands-on guidance, we help leaders across the country design, test, and scale solutions that build pathways for greater opportunity.
Your support makes this possible.